Achalasia:
Surgery has increased in popularity for achalasia following the advent of laparoscopic surgery. Previously the sugery required massive incisions with consequent pain and long recovery periods. The alternative non surgical options have an unpredictable and usually transient effect on the dysphagia. These non surgical measures include:
- Drugs
- Botox injections
- Forced balloon stretching
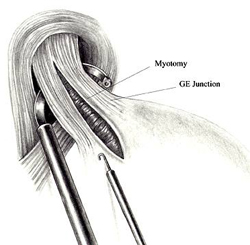 The surgical procedure most commonly perormed is a laparoscopic Heller's cardiomyotomy.
The surgical procedure most commonly perormed is a laparoscopic Heller's cardiomyotomy.
In this procedure the instrument placement is similar to that of a fundoplication.
The muscle fibres of the lower oesophagus are divided with care to avoid damaging the lining mucosa of the gullet.
This removes the obstruction to food and liquid passing into the stomach.
Nothing can be done for the lack of contractions in the upper part of the oesophgus and swallowing is aided by gravity alone.
As the sphincter at the bottom of the oesophagus is now eliminated it is likely that the patient will suffer from reflux of stomach contents into the oesophagus.
To help control the consequent reflux an antirflux fundic wrap is formed.
This is generally an anterior 180 degree wrap to minimise the degree of dysphagia induced by an antireflux procedure whilst affording protection against reflux of stomach contents.